
Tobacco use remains the leading preventable cause of death, disease, and disability in the United States1 and remains a significant public health concern. Roughly one in five American adults are currently smokers and half will die prematurely from smoking-related causes.1 Cigarette smoking, or nicotine use, adversely affects nearly all tissues and systems in the body. Many people are well aware that tobacco use increases the risks for cancer, lung diseases, heart disease, stroke, and depression, however, many people are surprised to learn that smoking damages the spine, contributing to intervertebral disc disease and facilitating osteoporosis.
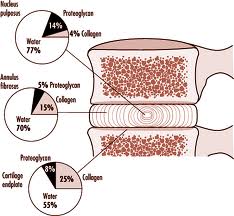
An intervertebral disc connects one vertebral bone to the next. The discs are the shock-absorbing cushions between each vertebra of the spine. The disc is made up of three basic structures: the annulus fibrosus, the nucleus pulposus, and the vertebral endplates. All three disc structures are made of different percent compositions of proteoglycan (proteins that bind water), collagen (the main protein in connective tissue), and water. The varying compositions create different functions. All these properties make the disc unique and highly specialized.
ANATOMY OF THE INTERVERTEBRAL DISC
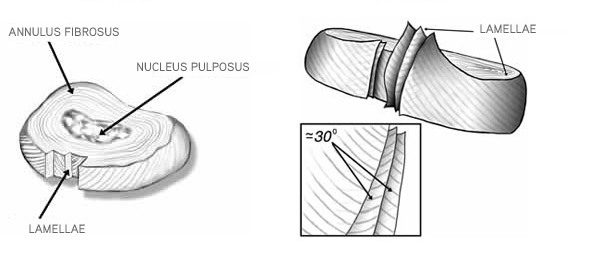
Each disc has a strong outer ring of fibers, called the annulus fibrosus. The annulus is comprised of specialized sheets of connective tissue, called lamellae, which are layered for strength. The annulus has a high amount of collagen that makes the outer layer extremely stiff. The nucleus pulposus is the soft, jelly-like center. It serves as the main shock absorber and is held in place by the outer annulus. The nucleus consists of a gel-like matrix that provides maximum hydration. It functions to distribute pressures in all directions within each disc under compressive forces.
The intervertebral disc is essential for providing spinal stability and proper alignment, withstanding compressive shock forces, and allowing for movement between vertebral bones. Discs in the spine increase in size from the neck to the low back as there are increasing needs for shock absorption due to weight and gravity. The intervertebral disc is an avascular tissue, meaning it does not naturally have a blood supply. Capillaries from the surface of the vertebral bodies supply the disc with nutrients. Thus, the disc is dependent on the blood supply to the vertebral bones.Nutrients & Nicotine
It is important to understand the effects nicotine and cigarette smoke have on the body. Tobacco smoke contains more than 7,000 chemicals with at least 250 known harmful chemicals, many of which are cancer-causing.2  Nicotine is naturally derived from the tobacco plant and attaches to nicotinic receptors in the body found in the central nervous system, autonomic nervous system, and neuromuscular junctions.3 Nicotine is largely responsible for the addictive properties associated with cigarette smoke.3 Smoking affects the entire body. Nicotine enters the blood supply and is rapidly distributed to most body tissues. Cigarette smoking is a leading cause of structural and functional changes in the cardiovascular system. Smoking causes injury and inflammation to blood vessels, decreasing essential blood flow to all tissues. This injury promotes the development of dangerous plaque and blood clots. Not only is the body’s major circulation compromised but so is blood flow to the intervertebral disc. Smoking also impairs collagen formation, one of the necessary structural proteins of the disc. Smoking literally prevents proper essential nutrients from reaching the discs and prevents adequate healing. These processes cause discs to prematurely degenerate and become diseased.
Nicotine is naturally derived from the tobacco plant and attaches to nicotinic receptors in the body found in the central nervous system, autonomic nervous system, and neuromuscular junctions.3 Nicotine is largely responsible for the addictive properties associated with cigarette smoke.3 Smoking affects the entire body. Nicotine enters the blood supply and is rapidly distributed to most body tissues. Cigarette smoking is a leading cause of structural and functional changes in the cardiovascular system. Smoking causes injury and inflammation to blood vessels, decreasing essential blood flow to all tissues. This injury promotes the development of dangerous plaque and blood clots. Not only is the body’s major circulation compromised but so is blood flow to the intervertebral disc. Smoking also impairs collagen formation, one of the necessary structural proteins of the disc. Smoking literally prevents proper essential nutrients from reaching the discs and prevents adequate healing. These processes cause discs to prematurely degenerate and become diseased.
In addition to damaging the disc, smoking has many other ill effects in the body.4
- Cancer
- Pregnancy complications including premature birth, death, and low birth weight
- Heart and blood disease
- Respiratory diseases
- Early menopause
- Erectile dysfunction
- Stained teeth and bad breath
- Gum disease and tooth decay
- Premature wrinkles
- Dementia and Alzheimer’s Disease
- Osteoporosis and increased fracture risk
DEGENERATIVE DISC DISEASE
The association between back pain and smoking in adults is well established by decades of research. Degenerative disc disease is a condition where vertebral discs are weakened; they no longer properly act as cushions between the vertebrae. Instead of remaining strong, the discs become softer. This condition can develop naturally as part of the aging process but may also result from injury. Disc degeneration is thought to be largely responsible for back pain.3 Degenerative discs typically begin with small annular tears. Just like other injuries, the tears heal by creating scar tissue, which is not as strong as the original disc wall. Over time, the process of tearing and scarring continually weakens the disc wall. In addition, as people age the hydrated nucleus becomes damaged and loses its water content. This fluid maintains needed pressures to act as a functional shock absorber. The nucleus can collapse and allow the vertebral bones to slide closer together with improper alignment. In time, improper alignment and arthritic changes can create bone spurs, herniated discs, pinched nerves, and spinal stenosis, all leading to pain.
Nicotine use may be directly responsible for intervertebral disc degeneration by causing cell damage in the annulus and nucleus.3 Evidence suggests that nicotine may have a direct toxic effect on the nucleus cells.3 This impacts the long-term health of the disc and its functional ability. All these detrimental changes mean that smokers damage not only healthy discs but greatly accelerate disc degeneration in any already damaged discs.
Smoking may also increase sensitivity to pain by altering the perception of pain through the neuroendocrine system.5 One study evaluated self-reported health statuses from over 25,000 patients and found smokers who had spinal symptoms for the same amount of time as non-smokers reported symptoms as more severe and present for a greater percentage of time each day.5 A dose-dependent relationship may exist where the risk for developing low back pain increases with the amount smoked.
OSTEOPOROSIS
Osteoporosis means “porous bone” and is a bone-thinning disease characterized by losing too much bone or not making enough new bone. This loss of bone mass leads to fragile bones that are more susceptible to fractures.
The National Osteoporosis Foundation estimates that 9 million Americans have osteoporosis and 48 million have low bone density.6 Because of the widespread prevalence and increased risk for fractures, approximately one in two women and up to one in four men over 50 years old will break a bone due to osteoporosis.6 Spinal fractures are the most common type of osteoporotic fractures. While osteoporosis has many risk factors contributing to its development, there is a strong association between smoking and osteoporosis.7 One study found that women who smoked more than one pack per day throughout adulthood had an average of 5-10% lower bone density than non-smokers in the low back by the time of menopause.7 Even secondhand smoke has been shown to negatively affect bone mineral density.7 Smoking clearly has a role in increasing the loss of bone density in all bones and the rate of loss is related to the daily number of cigarettes smoked and years of exposure. This is an independent risk factor from other factors that contribute to bone health such as sex, age, weight, BMI, and unhealthy lifestyle habits. For smoking alone, the lifetime risk of developing a spinal fracture is increased by 32% in men and 13% in women.7 Smoking also delays fracture healing. This is likely due to the fact that the toxic activity of nicotine stops the growth of cells essential for healing and reduces needed blood and oxygen supply.7 This is important not only for fracture healing but for any healing after a surgery.
NICOTINE USE & SPINAL SURGERY
Smoking negatively affects bone healing and the success rates in spinal surgery.3 Decades of research show that smokers have significantly poorer spinal surgery outcomes than non-smokers.5 Smokers experience higher rates of delayed wound healing, postoperative infections, and decreased successful spinal fusions than non-smokers.5 Smokers stay in the hospital longer and consume more hospital resources.7 One study looked at nearly 300 spinal fusion patients and found smokers were almost three times as likely to have a nonunion (failure to completely fuse) than non-smokers.5 The incidence of delayed wound and fusion healing is so significant that many surgeons feel proceeding with an elective fusion surgery would not be worth the risk while the patient is still smoking.7
QUIT TODAY
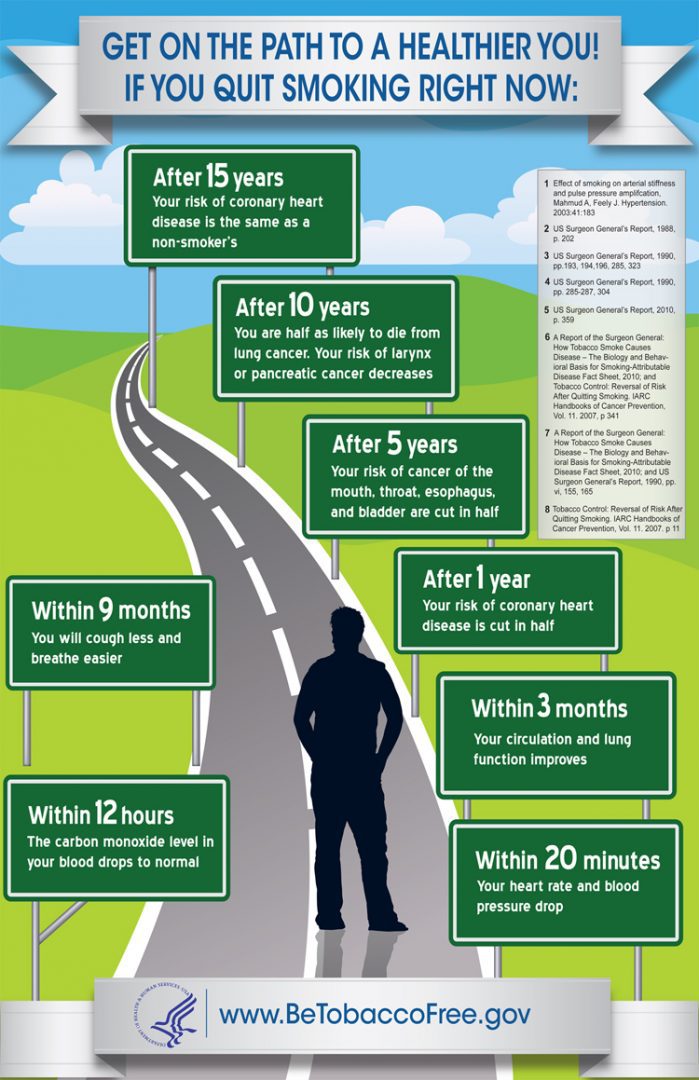
Smoking cessation is strongly advised. Positive and immediate improvements can be seen. Complete cessation can improve the healing process, reduce post-operative complications, and decrease the hospital stay. Even stopping five to seven days before surgery favorably increases wound healing.7 From just days to decades after quitting, your body continues to become healthier.
Easier said than done, quitting smoking is hard. The National Cancer Institute recommends these five steps be the START of every successful plan to quit smoking.8
- Set a quit date.
- Tell family, friends, and co-workers you plan to quit.
- Anticipate and plan for the challenges you will face while quitting.
- Remove cigarettes and other tobacco products from your home, car, and workplace.
- Talk to your doctor about getting help to quit.
If you are someone who has back pain or disc disease, quit now and improve your life. Your spine will thank you.
REFERENCES
- Centers for Disease Control and Prevention. Smoking and Tobacco Use: Fast Facts. Updated June 2013. Available from: http://www.cdc.gov/tobacco/data_statistics/fact_sheets/fast_facts/index.htm
- National Cancer Institute. Harms of Smoking and Health Benefits of Quitting. Available from: http://www.cancer.gov/cancertopics/factsheet/Tobacco/cessation
- Akmal M, Kesani, A, Anand B, et al. Effect of Nicotine on Spinal Disc Cells: A Cellular Mechanism for Disc Degeneration. Spine. Mar 2004;29(5):568-75.
- National Cancer Institute. Harms of Smoking and Health Benefits of Quitting. Reviewed 2011. Available from: http://www.cancer.gov/cancertopics/factsheet/Tobacco/cessation
- Vogt MT,Hanscom B, Lauerman WC, Kang JD. Influence of smoking on the health status of spinal patients: the National Spine Network database. Spine. Feb 2002;27(3):313-9.
- National Osteoporosis Foundation. What is Osteoporosis? National Osteoporosis Foundation Website. Available from: http://www.nof.org/articles/7
- Abate M, Vanni D, Pantalone A, Salini V. Cigarette smoking and musculoskeletal disorders. Muscles Ligaments Tendons J.Apr-Jun 2013;3(2):63–69. Published online 2013 July 9. doi: 11138/mltj/2013.3.2.063
- 5 Steps to START. NIH MedlinePlus: the magazine [Internet]. 2011 Winter [cited 2013 Aug 26];5(4):5. Available from: http://www.nlm.nih.gov/medlineplus/magazine/issues/winter11/articles/winter11pg5


